
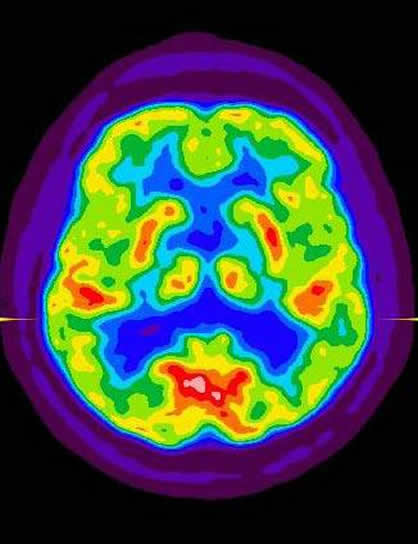
 The Journal of American Medical Association (JAMA) recently published a study on the viability of early surgical therapy for drug-resistant temporal lobe epilepsy.
The Journal of American Medical Association (JAMA) recently published a study on the viability of early surgical therapy for drug-resistant temporal lobe epilepsy.
Why surgery?
Jerome Engel, Jr., MD, PhD, along with 13 other leaders in the field of Neurology have taken on the issue of why, despite reported success, surgery for pharmacoresistant seizures is often seen as a last resort. Patients are typically referred for surgery after 20 years of seizures, often too late to avoid significant disability and premature death.
The group sought to determine whether surgery soon after failure of 2 antiepileptic drug (AED) trials is superior to continued medical management in controlling seizures and improving quality of life. The team had intended to enroll 200 participants, but the trial was closed earlier than anticipated due to slow enrollment of participants.
The Conclusions
The conclusions were that among patients with newly intractable disabling MTLE, resective surgery plus AED treatment resulted in a lower probability of seizures during year 2 of follow-up than continued AED treatment alone.
The Caveat
However, given the premature termination of the trial, the team has recommended that the results should be interpreted with appropriate caution.
Background on the Lead
Engel is Director of the Seizure Disorder Center, The Jonathan Sinay Distinguished Professor of Neurology, Neurobiology, and Psychiatry and Biobehavioral Sciences, and a member of the Brain Research Institute at UCLA. Engel’s bibliography lists over 1,000 publications and 30 books, including Epilepsy: A Comprehensive Textbook, Surgical Treatment of the Epilepsies, and The Treatment of Epilepsy. He is also the principal investigator on three research grants from the National Institute of Neurological Disorders and Stroke.





Charles Marshall
Hi Jessica,
Thank you for your blog and this article. The doctor mentioned the S-word for the first time today as he switched my daughter’s medication from Keppra (which we tried for over two years unsuccessfully) to Trileptal. We are going to wean her off the Keppra and gradually introduce the Trileptal. If it doesn’t work there is a possibility of surgery. Frankly, surgery scares the daylights out of me, so we’re praying the Trileptal works.
In regard to what I’d like to hear more about on your blog, my wife and I have found that my daughter's partial-complex seizures are almost all triggered by heat. This is especially true when she is in enclosed places, such as a hot shower, car, or even wrapped up in a blanket.
When she has the seizures, my wife and I immediately implement what we refer to as “cooling measures“ in order to bring her core temperature down. We lightly bath her back and limbs with a cold cloth, remove excess clothing, and place small bits of ice in her mouth (nothing she could choke on). These measures have served to arrest the seizures and bring her back around within no less than 2 minutes 100% of the times that we’ve applied them.
When we've mentioned this to doctors, they almost always look at us like we're at best, poor dumb parents, and at worst, out of our minds. Have you run across any people who have had heat-triggered seizures? I would be interested to hear their experiences. Once again, thanks for your blog.